
Simulating the Control Arm: Virtual Patients at the Trial Bottleneck
Digital twins promise smaller, faster trials, and the regulatory scaffolding is forming. But there’s still a validation gap.

Clinical trials remain the most expensive bottleneck in drug development. And although this stage comes after all the high tech pharmacological tinkering is over, a trial conduct runs into its own obstacles.
⚠️ The most immediate one is patient recruitment. Far back in 1979, the father of clinical pharmacology Louis Lasagna observed that the pool of eligible patients shrinks by 90% the moment a trial opens, only to reappear once it closes. Lasagna’s Law remains as relevant as ever: according to a 2022 article, 11% of trial sites enrol zero participants and nearly 90% of trials face meaningful delays. With Phase II and III trials costing roughly $40,000 per day, the financial toll is brutal.
⚠️ Another issue is clinical attrition. Research from VU Amsterdam found that between 2012 and 2019, the share of trials successfully completing each phase declined steadily—particularly at Phase II. In the first half of 2024, nearly a third (32%) of trials were discontinued at Phase II—a 56% rise compared to pre-pandemic levels. Combined with stagnant rates of Phase III initiation over that same decade, the picture is one of a systemic bottleneck: trials that begin are increasingly unlikely to see the finish line.
⚠️ Rare disease research presents its own distinct challenge. As the FDA’s Rare Disease Evidence Principles note, shrinking patient populations make it progressively harder to generate reliable efficacy data through conventional designs—especially placebo-controlled trials, where enrolling enough participants to reach statistical significance can be close to impossible.
⚠️ Apart from operational intricacies, there is the ethical dilemma. Randomized controlled trials remain the gold standard for evaluating new therapies, but randomization isn’t always defensible. When an effective treatment already exists, assigning patients to a placebo raises serious moral questions, e.g. HIV cure trials with the antiretroviral treatment interruption.
The question, then, is whether parts of the control process can be simulated rather than physically recruited.
Digital twins are emerging as a compelling response. Last October, Sanofi Ventures invested in a digital twin platform developer QuantHealth, bringing its total funding to $30M. In 2025, the FDA announced plans to phase out animal testing requirements for monoclonal antibodies in favor of human-relevant methods, including AI-driven computational models—with the EMA moving in the same direction. Both industry and regulators, it seems, are taking this technology seriously.
👥 How it Works
A digital twin is a virtual replica of a physical object, continuously updated with real-world data so it mirrors the original’s behavior in real time. The concept, first applied by NASA in the 1960s, has since migrated from engineering into healthcare.
The applications are wide-ranging: optimizing industrial processes as Eli Lilly did to boost production of their GLP-1 drugs, predicting equipment failures, streamlining supply chains, and accelerating product development.
In a clinical trial patients are generally divided into two groups, also known as arms. The intervention arm receives the experimental treatment; the control arm receives a placebo, standard-of-care treatment or sham, serving as the baseline against which results are measured. Randomized controlled trials (RCTs) are the gold standard because randomization minimizes bias, but that randomization isn’t always flawless.
The traditional workaround of external controls drawn from historical trials, health records, or registries all carry their own limitations. For instance, data like those don’t include underrepresented groups or don’t account for placebo effect due to their observational nature.
Digital twins go a step further: using AI models augmented with historical data, they generate individualized predictions of how a patient might respond under different treatment scenarios. When used to simulate outcomes for patients who do not receive the experimental therapy, these models can produce a synthetic control arm.
These trial-level twins build on a foundation of patient-specific digital twin modeling (virtual replicas of individual physiology shaped by genomics, imaging, and clinical history) which we covered in our earlier overview of biological and patient-specific twins.

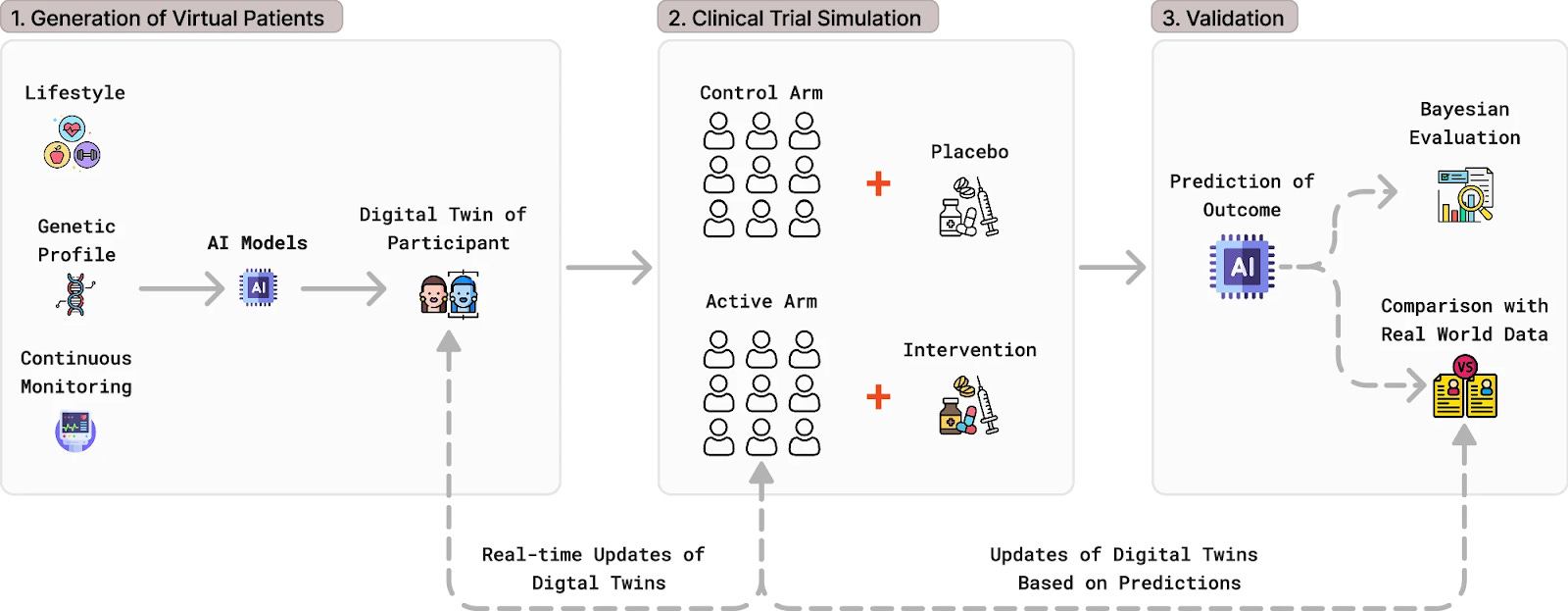
In clinical trials, an AI-powered digital twin typically operates in three steps:
Build virtual patients — AI integrates biomarkers, imaging, genetics, and real-world evidence to generate synthetic profiles capturing the full variability of real populations.
Run simulated trials — virtual cohorts replace placebo groups or test experimental therapies in silico, probing efficacy and safety without exposing patients to unnecessary risk.
Optimize continuously — trial parameters like dosing and sample size are continuously refined in real time, anchored by validation against real-world data.
A less computationally demanding synthetic control arm approach uses AI-generated patient data based on registries, and real-world evidence but unlike DTs not modelling it on a particular individual. The appeal is sharpest in rare diseases, where finding enough eligible control patients is often impractical. The FDA, EMA, and NICE have all endorsed the approach, and it’s gaining traction: recent Phase II/III myeloma and lymphoma trials have leaned on external control data, and in at least one case (blinatumomab for acute lymphoblastic leukemia), a synthetic control arm helped support accelerated regulatory approval. AstraZeneca used over 300M synthetic patient records to advance its clinical trials, allegedly saving up to $100M per drug in development.
Synthetic control arms built from historical data have already supported label expansions and accelerated approvals with alectinib, blinatumomab, palbociclib among them. AI-generated individualized digital twins, however, have not yet served as primary evidence in a completed approval.
🦾 An Industry Arm
Business models in this space vary significantly. Some companies license their platforms as SaaS tools to sponsors (Unlearn, Phesi), others embed digital twin capabilities within broader trial-management suites sold enterprise-wide (Medidata), and a few operate closer to a service model, generating synthetic data or external control arms on a per-study basis (ConcertAI).
The clearest commercial traction spans two approaches: prognostic covariate adjustment, which uses digital twins to shrink control arms within standard RCTs, and synthetic control arms, which replace part or all of the control group with external or simulated data.
⭐ Unlearn.ai’s PROCOVA method (EMA-qualified, with positive FDA feedback) embeds prognostic scores from digital twins directly into Phase 2/3 trial design. The company has worked with AbbVie and J&J on Alzheimer’s trials and partnered with Quralis and ProJenX for ALS, and raised $50M in a 2024 Series C. Notably, the EMA qualification covers the statistical adjustment procedure and applies only to trials with continuous outcomes, not the AI model-building step itself.
⭐ Phesi approaches the same problem from a data-scale angle, drawing on a clinical database surpassing 132M patients to construct digital twins that, as a milestone proof-of-concept study showed, can replicate standard-of-care arms in cGvHD trials—work that earned it recognition as a Frost & Sullivan Global Growth Leader in AI-enabled clinical trials.
⭐ Medidata, backed by Dassault Systèmes, offers synthetic control arm technology as part of a full-stack platform spanning 38,000+ studies; it recently extended its partnership with Sanofi for decentralized trials, and Anthropic’s Claude for Healthcare now includes a Medidata connector.
⭐ ConcertAI rounds out the trial-support layer, structuring real-world data from 11M+ patients into external comparator arms, now running on NVIDIA infrastructure after a 2024 integration agreement, and partnering with Bayer on multiomic cancer data.
💊 Drugs Before Trials
Before a trial even begins, a patient’s virtual replica can simulate treatment effects entirely in silico. That potential extends across every major stage of drug development:
Early discovery: model disease mechanisms and surface therapeutic targets through biological simulation rather than empirical screening alone.
Preclinical testing: simulate human responses to reduce reliance on animal models while generating more clinically predictive data.
Clinical trial simulation: stress-test doses, treatment plans, and patient selection criteria on virtual cohorts before recruiting real ones.
Regulatory submissions: supply in silico safety and efficacy evidence alongside clinical data, with review bodies increasingly weighing DT-specific concerns like model bias and algorithmic transparency.
Post-market surveillance: continuously update with real-world data to monitor drug safety and efficacy after approval.
⭐ Aitia uses its causal REFS engine to model disease biology from multiomics data and simulate clinical outcomes entirely in silico, bypassing animal and cell-line models. The platform spans neurodegeneration, oncology, cardiometabolic disease, and immunology, validated by a 2024 partnership with Orion in oncology drug discovery, an extended agreement with Servier on brain cancer, and a 2025 partnership with Gustave Roussy to map biological causes of human cancer.
⭐ VeriSIM Life takes a pharmacokinetic angle: its BIOiSIM platform uses hybrid AI and mechanistic modeling to predict drug behavior in humans before trials begin, scoring compounds on a Translational Index (essentially a credit score for drug viability) across a search space of over one trillion compounds and 5,000+ validation datasets, claiming a 2.5-year average reduction in time to IND.
⭐ Also operating at the patient level: Orakl Oncology, a 2023 Gustave Roussy spin-off we covered previously, builds tumor avatars from patient samples to simulate drug responses and identify therapeutic targets, and raised €11M in 2024 seed funding.
🚧 Unavoidable Limitations
Despite obvious promise in clinical trials and drug development, digital twins face challenges as a technology. The Unlearn.AI’s team highlights four key limitations of the approach:
Complexity and variability: Unlike mechanical systems, each patient has a unique biological profile shaped by genetics, environment, and lifestyle. Human physiology operates through dynamic, nonlinear interactions that are difficult to simulate — requiring novel AI architectures, robust validation procedures, and continuous model updating as standards of care evolve.
Data availability and standardization: DT models must integrate health data from disparate sources. EHRs are abundant but inconsistent and heterogeneous, while clinical trial data is high-quality but limited in scale and population representativeness. Building globally representative datasets remains a massive challenge, compounded by data drift, changing measurement standards and socioeconomic factors. The input requirements for a credible trial-level twin (longitudinal biomarkers, imaging, genomics, lifestyle data) often exceed what trial sites currently capture at the point of care. Compounding this, clinical data standards remain fragmented: CDISC (FDA’s mandated submission format) was designed for traditional RCTs over twenty years ago and does not natively accommodate real-world data or non-interventional designs, while FHIR and OMOP offer better support for EHR and observational data but lack regulatory adoption as submission standards.
Prognostic value and validation: Predicting individual responses to treatment is difficult given the complexity of biological interactions and frequent data gaps. AI models must handle missing data, diverse data types, and outcome distributions — all while maintaining clinical-grade precision. Robust, context-aware validation is essential but resource-intensive.
Ethical and privacy concerns: Patient data is sensitive and heavily regulated. Key concerns span data collection, management, analysis, and use — including cybersecurity risks, algorithmic bias, and the need for transparent, continuously monitored models to ensure equitable outcomes.
🔭 Regulations and Lookahead
The regulations agencies are picking up the pace with respect to digital twins. In the US, while DTs are still not recognized as a tool, a 2024 collaboration between the NSF, NIH, and FDA is exploring this technology as a catalyst of biomedical innovation and their potential to transform preclinical and clinical research.
A Center for Drug Evaluation and Research (CDER) discussion paper, originally published in 2023 and updated in 2025, further outlined current and future applications of digital twins, highlighting their potential to accelerate drug development and support placebo arm replacement.
In case of a placebo control arm, no fundamental barriers exist: sponsors wishing to use a digital twin in place of a placebo control arm must notify the FDA at the IND filing stage and provide consistent, transparent updates throughout the trial.
In Europe, the EMA has taken concrete steps as well. In late 2022, its CHMP issued a Qualification Opinion for Unlearn’s PROCOVA. This was followed by the EMA’s five-year AI Action Plan, committing to technical deep dives into digital twin technology among other tools. Broader AI governance in the medical space is also addressed under the EU AI Act.
Checking back with our 2025 review, the European Commission’s Virtual Human Twins Initiative, backed by over €100 million in combined Horizon Europe/Digital Europe funding, has moved past the manifesto stage since last year. The EDITH coordination action published its strategic roadmap and policy brief in October 2025, and in June 2025 the Commission launched procurement for the VHT digital platform that will host model integration and validation. The Manifesto itself has grown to over 100 signatories by now, and the infrastructure is now being built.
Outside the US and EU, regulatory engagement is more tentative, a few instances:
Japan’s PMDA has published an AI Action Plan and launched ‘Early Consideration’ publications to address emerging technologies in drug development, though it has not yet issued digital twin-specific guidance.
In China, the NMPA’s 2022 Technical Review Guidelines for AI Medical Devices require that AI tools demonstrate data sufficiency, diversity, and representativeness, and mandate that self-learning algorithms be “locked” post-market unless resubmitted for review, a rules-based approach that some contrast with the more standards-oriented frameworks in the US and EU. Like Japan, China has not yet extended this framework to digital twin methodology as a distinct category.
Both agencies are modernizing, but neither appear to have matched the EMA’s qualification-level endorsements or the FDA’s explicit discussion-paper engagement with DT methodology.
Early examples like Phesi’s cGvHD work suggest that digital twins can already strengthen evidence generation in specific settings. The more plausible near-term future, however, is not a fully virtual clinical trial, but a hybrid model in which computational controls gradually replace or reduce traditional placebo arms where they are hardest to justify.
It should be noted we haven’t gone into questions like the commercial model, whether SaaS licensing, per-study pricing, or platform embedding will prove most durable, nor into how HTA bodies like NICE or IQWiG would weigh DT-generated evidence in reimbursement decisions. Both will shape adoption as much as the technology itself.